Ross & Baruzzini Team Secures Rare Copy of the Declaration of Independence
Article was originally published on July 1, 2016. Updated on June 30, 2022. On…
 When UPS relocated its worldwide headquarters to the Atlanta, Georgia, area in 1992, Kinser & Associates Consulting Engineers was hired to provide technology consulting and design for over 750,000 SF of office space requiring over 2,800 voice and data drops through a structured and flexible cabling system. This project inspired Don Kinser to pivot. He formed Environmental Design International (EDI) as an IT consulting and design firm.
When UPS relocated its worldwide headquarters to the Atlanta, Georgia, area in 1992, Kinser & Associates Consulting Engineers was hired to provide technology consulting and design for over 750,000 SF of office space requiring over 2,800 voice and data drops through a structured and flexible cabling system. This project inspired Don Kinser to pivot. He formed Environmental Design International (EDI) as an IT consulting and design firm.
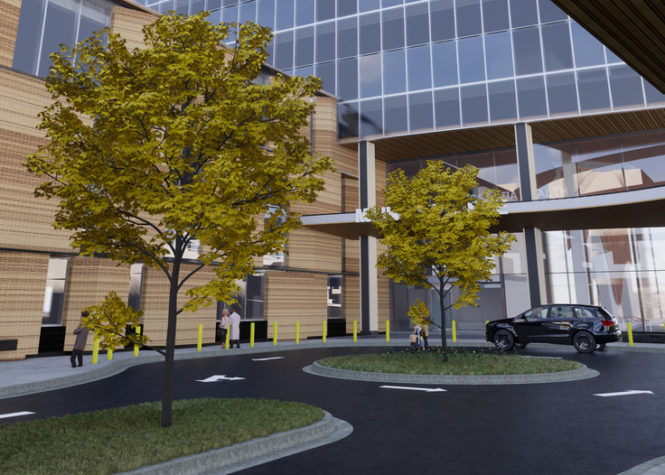
Building on this foundation and thousands of projects since its founding, EDI understands that efficient and effective technology solutions are critical when planning and designing today’s advanced corporate facilities. Supporting projects around the world, we provide advisory services, technology system design, data center-specific services, and technology program management for various types of technology projects in the healthcare, corporate, education, and other markets.
In 2018, Ross & Baruzzini acquired EDI, Ltd. Craig Toder, Ross & Baruzzini chairman, said at the time “EDI is a very respected consulting firm specializing in design and program management of information technology, audio/visual, security, and other technology systems. This will add capabilities we’ve wanted to better serve our markets and provide a broad platform for EDI’s long-term growth.”
Don Kinser, EDI’s founder and chairman of the board, said the acquisition provides EDI with exciting benefits for its clients and employees. “We are thrilled to be part of a forward-thinking global organization with a long-trusted history in the industry. Our exciting new partnership provides great value to our clients and tremendous opportunities for our employees.”
 Don Kinser, Founder
Don Kinser, Founder
After graduating from Georgia Tech, Kinser worked at small engineering firms while earning a Professional Engineer (PE) registration. With that in hand, he formed Kinser & Associates Consulting Engineers (KACE) in 1986, along with Dan Clifford and Joe Milam. Through two strategic hires, John Sams in 1990 and Jim Harrison in 1991, KACE had the right array of technology service experts to form Environmental Design International, Ltd., later shortened to EDI.
![]()



“The EDI team were essential in helping Georgia Tech develop a sound technology vision for our High Performance Computing Center. They led the effort to gather technical requirements from investigators, faculty, OIT, and industry partners. (They) developed multiple models forecasting data center growth for both research and administration institutional needs and advised us on leading data center design approaches and alternatives.”

“EDI is a world-class medical systems designer. Modern healthcare systems require integration and knowledge of the latest technologies to support the staff and serve the patients. EDI is our solution for this.”

“Over the past three years, Memorial Health Care Systems (MHCS) has had the opportunity of working with EDI on our Master Facility project. The experience and support that EDI brought to the team was invaluable. Many complex and antiquated systems created many challenging opportunities, since most could not be interrupted for any amount of time. When MHCS implements their next growth strategy, EDI will be a preferred consultant and team member.”
Let our teams of engineers, designers, planners, and visionaries guide your future project into lasting, sustainable success. Talk to an expert today.

Article was originally published on July 1, 2016. Updated on June 30, 2022. On…

Director of Corporate Strategy and Innovation, Chris Runde, was excited to take part in…

Security Systems News’ (SSN) monthly column, Specifically Speaking, features Dan Mike, Principal – Director…

Ross & Baruzzini Security Vice President – Managing Principal, Phil Santore, spoke with Security Magazine on how…

Integral Group, a global network of deep green engineers and consultants, and Ross &…